Medicine likes to present itself as a field of answers, but some of the strangest questions about our own bodies remain stubbornly open. Even with whole human genomes sequenced, AI scanning our scans, and lab tests for almost everything, there are conditions doctors still cannot fully explain, predict, or cure. For patients, these mysteries are not abstract puzzles – they are daily reality, often filled with fear, uncertainty, and trial‑and‑error care. For scientists, they are maddening and irresistible at the same time, hinting that our understanding of biology is still only partial. These ten unsolved medical mysteries show just how much we do not yet know about being human, and why that ignorance matters.
The Brain on Fire: Why Some Immune Systems Suddenly Attack the Mind
One of the most unsettling modern mysteries in medicine is autoimmune encephalitis, sometimes called the “brain on fire” syndrome. In these cases, a person who seemed perfectly healthy can suddenly become paranoid, hallucinate, have seizures, or slip into catatonia in a matter of days or weeks. Doctors now know that, in some patients, antibodies are attacking receptors on brain cells – especially receptors for glutamate and other neurotransmitters – but they still do not fully understand what triggers this immune rebellion. In many documented cases, a tumor or infection seems to set off the chaos, but in a large share of patients, no clear cause is ever found. The terrifying part is that the condition can initially look like a psychiatric crisis, so people may be misdiagnosed with schizophrenia or bipolar disorder instead of a treatable immune disease.
When caught early, high‑dose steroids, immune‑suppressing drugs, and even blood‑filtering treatments can bring people back from the brink, sometimes almost completely. Yet others are left with lasting memory gaps, personality changes, or epileptic seizures even after the antibodies have dropped. Why one person’s immune system turns on their brain at twenty and another’s never does remains an open question. Researchers suspect a mix of subtle genetic risk, environmental triggers, and viral exposures that may have happened years before symptoms. That blend of science and uncertainty makes every new case both hopeful, because treatments exist, and haunting, because the underlying switch that flips from normal to attack mode is still invisible.
Long COVID and ME/CFS: The Post‑Viral Puzzle No One Can Solve
For decades, people living with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) were dismissed as anxious, depressed, or simply “burned out.” Then Long COVID arrived and forced the medical world to confront an uncomfortable truth: viruses can leave behind long‑lasting, debilitating syndromes that modern tests still struggle to capture. Millions around the globe now report crushing fatigue, brain fog, unrefreshing sleep, dizziness on standing, and strange heart‑rate swings months or even years after a coronavirus infection. The similarity to classic ME/CFS symptoms is striking, yet there is still no single biomarker, no definitive scan, and no widely accepted mechanism that ties it all together. Hypotheses range from smoldering viral fragments and immune system overdrive to microclots in tiny blood vessels and damage to the autonomic nervous system.
What makes this mystery especially painful is its scale. Roughly about one in ten people after a symptomatic COVID infection seem to develop some form of prolonged symptoms, though estimates vary by study and country. Despite intense research, treatments remain mostly supportive: pacing activities, managing sleep, trying medications one by one, and hoping the body slowly resets. This stands in sharp contrast to acute viral infections, where specific antivirals or vaccines can be targeted with sniper‑like precision. The post‑viral world is more like a foggy battlefield where cause and effect are blurred. Until scientists can decode why some bodies never fully “turn off” the alarm after infection, millions will remain stuck in limbo between illness and official understanding.
The Placebo Effect: How Fake Treatments Sometimes Work Better Than Real Ones
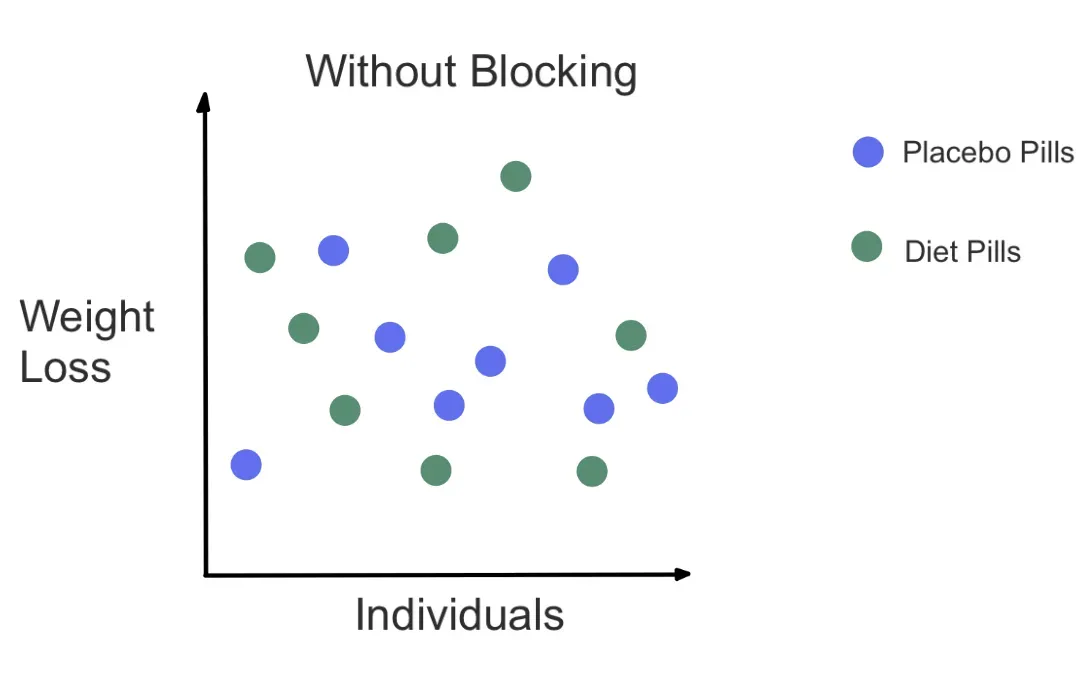
Few medical mysteries are as philosophically unsettling as the placebo effect. People given a sugar pill, a saline injection, or even a sham surgery – when done ethically in research – can experience real pain relief, better sleep, fewer hot flashes, or improved mood. Brain imaging studies show changes in pain networks, dopamine release, and even immune markers when someone believes they are being treated. Yet, despite decades of research, medicine still cannot fully explain why belief and context can rival powerful drugs for some patients. It gets stranger: the color of a pill, the size of a tablet, and even the perceived confidence of a doctor can all influence how well a placebo seems to “work.”
One of the most surprising findings is that placebos can still have an effect even when people are told they are taking a placebo, as long as it is framed as something that might help by harnessing mind‑body connections. That raises uncomfortable questions about how much of standard care is driven not only by the drug itself, but also by the story wrapped around it. At the same time, the placebo effect cannot cure cancer or mend a broken bone; its power has limits that remain blurry but real. The ethical line is also a puzzle: how can doctors ethically use placebo power without deceiving patients? Understanding this strange effect better could help design treatments that maximize real drug effects and supportive context together, but the underlying biology of belief is still largely uncharted territory.
Spontaneous Remission: When Deadly Diseases Vanish Without a Clear Reason
In the age of precision oncology and targeted therapies, the idea that a serious cancer can shrink or disappear on its own sounds like myth. Yet there are carefully documented cases where aggressive leukemias, lymphomas, or even melanomas have gone into remission without conventional treatment, or after only minimal intervention. Doctors suspect that, in some of these rare cases, the immune system suddenly recognizes the tumor as dangerous and mounts a fierce attack, sometimes after a strong infection or an unrelated immune jolt. But in many recorded remissions, there is no obvious spark that explains why one person’s disease vanished while another’s progressed. These cases are rare – representing only a tiny fraction of overall cancer outcomes – but they haunt oncologists because they suggest our current models of cancer behavior are incomplete.
Researchers are trying to reverse‑engineer these miracles, sequencing tumors before and after remission when samples exist, and looking for unusual T‑cell responses or viral footprints. There is hope that studying spontaneous remission might inspire new immunotherapies that coax the body into repeating the same trick on demand. Still, the data are patchy, and by definition, these events are hard to predict and therefore hard to study systematically. For patients and families, stories of sudden remission can be emotionally double‑edged: they inspire hope but can also feed unrealistic expectations. The mystery is not just why remission happens but why it happens so rarely. Until that pattern is cracked, spontaneous remission will remain one of medicine’s most tantalizing outliers.
Fibromyalgia and Chronic Pain: When the Nervous System Becomes a Black Box
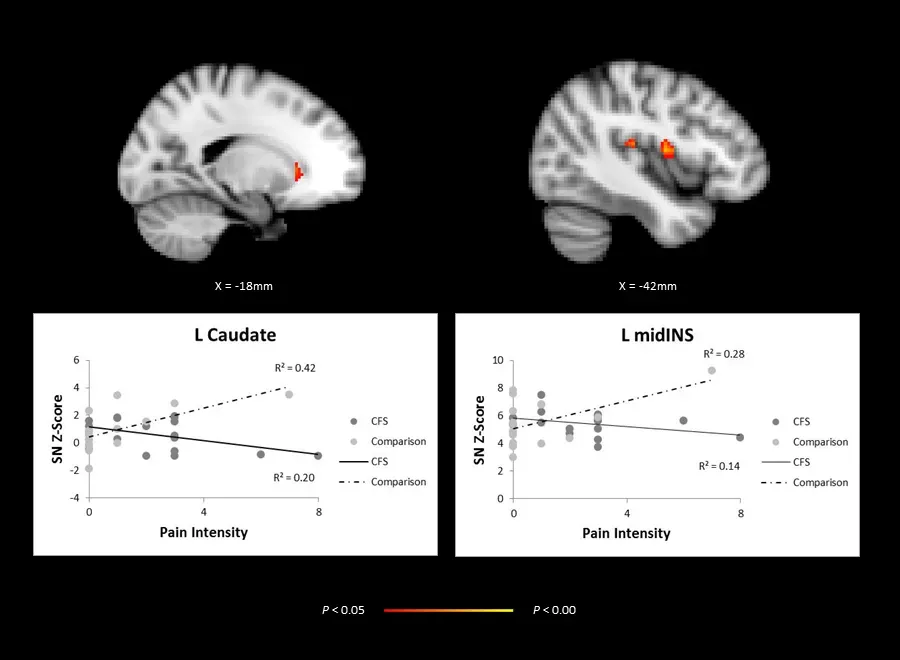
Fibromyalgia sits at the crossroads of neurology, rheumatology, and psychiatry, and no field fully owns it. People diagnosed with fibromyalgia often describe widespread body pain, deep fatigue, and foggy thinking, yet traditional tests – X‑rays, blood work, even standard nerve studies – often come back looking completely normal. Some brain imaging studies reveal heightened responses to pain signals, as if the volume knobs in the central nervous system are turned up too high. Other research points to subtle changes in small nerve fibers, immune signaling, or sleep architecture, but none of these findings has crystallized into a simple diagnostic test. The result is that many patients are left fighting not only their symptoms but also lingering doubt from employers, insurers, and sometimes even clinicians.
Chronic pain more broadly faces the same knowledge gap. Two people with nearly identical MRI findings of a spinal disc problem can have wildly different levels of pain, and no one can yet predict reliably who will suffer the most. Treatment often involves a frustrating carousel of medications, physical therapy, psychological support, and lifestyle adjustments, with mixed success. The traditional “find the damaged tissue, fix the tissue” model of medicine breaks down when the problem seems to be in the way the nervous system processes signals rather than in a single obvious injury. This has pushed scientists to rethink pain as a complex brain‑body system rather than just a symptom. But until the field can translate that complexity into accurate tests and targeted therapies, chronic pain will remain one of medicine’s most lived‑in mysteries.
Sudden Cardiac Death in the Young: When a Healthy Heart Simply Stops
Few medical events are as shocking as the sudden collapse of a teenager or young adult who seemed perfectly healthy minutes earlier. Sudden cardiac death in the young often occurs during sports or intense activity, and autopsies sometimes reveal hidden structural heart conditions like hypertrophic cardiomyopathy or coronary artery anomalies. In other cases, however, the heart looks structurally normal, and suspicion falls on subtle electrical disorders like long QT syndrome or Brugada syndrome, which can disrupt the heart’s rhythm without leaving clear structural scars. Genetic testing has uncovered risk variants in some families, but in a significant portion of cases, no definitive cause is ever found. For grieving parents, the lack of an answer compounds the loss.
Screening young athletes with electrocardiograms and echocardiograms has been proposed and adopted in some countries, but the approach remains controversial. False positives can sideline healthy kids and create anxiety, while false negatives give a false sense of security. There is also the haunting problem of so‑called “idiopathic” cases, where every test available today comes back inconclusive. This mystery forces cardiology to confront the limits of current technology: there are almost certainly electrical and molecular abnormalities we do not yet know how to detect. The tragedy is that in many of these conditions, a simple implanted defibrillator or lifestyle adjustment could be lifesaving if only the risk could be identified in time. Until medicine can see further into the heart’s invisible wiring, some sudden deaths will remain unsolved.
The Gut–Brain Axis: How Microbes Might Shape Mood, Cravings, and Disease
It is hard to think of a more surprising plot twist in modern medicine than the rise of the gut microbiome from obscure niche to starring role. Trillions of microbes in the digestive tract help break down food, train the immune system, and produce molecules that interact with hormones and nerves. Studies have linked differences in gut flora to obesity, inflammatory bowel disease, and even mood disorders like depression and anxiety. Animal experiments show that transplanting gut microbes from one mouse to another can transfer not only metabolic traits but also behavioral tendencies. Yet, despite the hype, the field is still in its infancy, and doctors cannot yet look at a stool sample and give precise, actionable advice beyond very general patterns.
The so‑called gut–brain axis adds an extra layer of mystery. Nerves, immune cells, and microbial metabolites form a feedback loop that may influence appetite, stress responses, and even how people respond to certain medications. Fecal microbiota transplants can cure life‑threatening Clostridioides difficile infections in the vast majority of cases, suggesting that, in some contexts, simply changing the microbial community is as powerful as any drug. But when similar approaches are tried for more complex diseases, results are much more mixed and unpredictable. The hardest questions remain unanswered: which microbes matter most, in what combinations, for which person, at which moment in life? Until science can untangle that web, the gut–brain axis will remain one of the most tantalizing and over‑interpreted frontiers in modern medicine.
Why These Mysteries Matter: Cracks in the Story of “Settled” Science

It can be tempting to treat these conditions as edge cases, the strange anecdotes that do not change the big picture of medical progress. But each unresolved puzzle points to a deeper gap in how we think about the body. Traditional medicine excelled at treating single‑cause, single‑organ problems: a bacterial infection in the lung, a blocked coronary artery, a broken bone. It is far less comfortable with diffuse, systemic issues like post‑viral syndromes, chronic pain, or micro‑scale electrical disturbances. The unresolved nature of these mysteries forces a kind of humility, reminding us that even advanced imaging and genomics are not the same as full understanding.
These gaps also have real‑world consequences. When doctors cannot neatly explain a condition, patients often fall through cracks in insurance coverage, disability claims, and social support. Historical biases – like the tendency to psychologize symptoms more often in women – are amplified when objective tests are lacking. On the scientific side, unsolved problems are often where the next breakthrough hides; past revolutions in ulcer treatment, HIV care, and cancer immunotherapy all began with phenomena that did not fit the existing models. In that sense, mysteries are not embarrassing side notes but essential fuel for progress. The real danger is not that we do not know, but that we act as if uncertainty does not exist.
The Road Ahead: New Tools, Old Questions, and Global Stakes

Looking forward, many of these mysteries are likely to be cracked not by a single discovery but by combining new tools across fields. High‑throughput sequencing, for example, can scan immune cells in autoimmune brain disease or Long COVID patients to see which targets they are fixated on. Advanced neuroimaging may eventually map pain networks in enough detail to distinguish different chronic pain subtypes and guide more personalized treatment. AI systems are being trained to sift through massive health records and wearable data to find patterns that human clinicians might miss, such as early warning signals for sudden cardiac death. Each of these tools offers a new lens, but they also raise new questions about bias, privacy, and who gets access to cutting‑edge care.
The stakes are not just individual but global. Post‑viral syndromes can sap workforce participation and strain disability systems; chronic pain drives huge costs in lost productivity and opioid prescribing; misdiagnosed heart conditions can devastate families and communities. Emerging therapies – like engineered immune cells, microbiome‑targeted drugs, or bioelectronic implants that modulate nerve activity – could shift outcomes dramatically, but only if they are tested in diverse populations and not just in wealthy research hubs. At the same time, almost every breakthrough risks widening inequality if it is available only to those who can pay. The future of these mysteries, in other words, is not just about cracking biological codes but also about deciding whether the benefits of new knowledge are shared fairly.
What Readers Can Do: From Curiosity to Real‑World Impact
It is easy to read about unsolved medical mysteries and feel helpless, but individual choices actually matter more than most people realize. One simple, powerful act is to take symptoms seriously – your own and others’ – even when they do not fit a neat diagnosis. Listening without dismissing someone’s pain or fatigue as “just stress” can be a quiet form of advocacy. Supporting friends or family members navigating poorly understood conditions can also mean accompanying them to appointments, helping track symptoms, or encouraging second opinions when answers feel too thin. Curiosity can turn into compassion when we remember that behind every “mysterious case” headline is a real person trying to hold their life together.
Readers can also back the science directly and indirectly. That might mean participating in reputable research studies or patient registries, which are crucial for rare or complex conditions, or donating to organizations that fund work on ME/CFS, Long COVID, sudden cardiac death, or chronic pain. Learning to be a critical consumer of health news – questioning over‑simplified miracle cures and seeking out nuanced reporting – helps create demand for better science and better journalism. Even talking about these mysteries with kids, students, or colleagues can shift cultural expectations away from the idea that medicine already has all the answers. In a field defined by uncertainty, staying curious, skeptical, and humane is its own kind of contribution.

Suhail Ahmed is a passionate digital professional and nature enthusiast with over 8 years of experience in content strategy, SEO, web development, and digital operations. Alongside his freelance journey, Suhail actively contributes to nature and wildlife platforms like Discover Wildlife, where he channels his curiosity for the planet into engaging, educational storytelling.
With a strong background in managing digital ecosystems — from ecommerce stores and WordPress websites to social media and automation — Suhail merges technical precision with creative insight. His content reflects a rare balance: SEO-friendly yet deeply human, data-informed yet emotionally resonant.
Driven by a love for discovery and storytelling, Suhail believes in using digital platforms to amplify causes that matter — especially those protecting Earth’s biodiversity and inspiring sustainable living. Whether he’s managing online projects or crafting wildlife content, his goal remains the same: to inform, inspire, and leave a positive digital footprint.


